Last updated on Jul 20, 2026

CMS-1500 UB-04 CMS-1450 Package free printable template
We are not affiliated with any brand or entity on this form
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is CMS-1500 UB-04 CMS-1450 Package
The Health Insurance Claim Form is a vital document used by patients and healthcare providers to submit medical claims to insurance companies for reimbursement.
pdfFiller scores top ratings on review platforms
I have only been using a few days give me time and I will let you know.
its been a good one except when a have a parallel page and i need it to be vertical i cannot rotate it. (I tried)
You made it so easy and I did not have to pay my accountant to do it. Thank you.
It's easy to use, I do like it; but it is a little expensive, $80/year is a lot. I use it maybe once or twice per month. I think you would have more customers if it was less expensive.
I couldnt have been happier with any other product!! This is awesome!
Easy to learn and use, lots of features that are helpful for my business
Who needs CMS-1500 UB-04 CMS-1450 Package?
Explore how professionals across industries use pdfFiller.

CMS-1500 UB-04 CMS-1450 Package is needed by:
-
Patients seeking reimbursement for medical services.
-
Insured individuals who need to process health claims.
-
Physicians or suppliers providing medical services.
-
Healthcare administrators managing billing processes.
-
Insurance companies reviewing claim submissions.
Comprehensive Guide to CMS-1500 UB-04 CMS-1450 Package
What is the Health Insurance Claim Form?
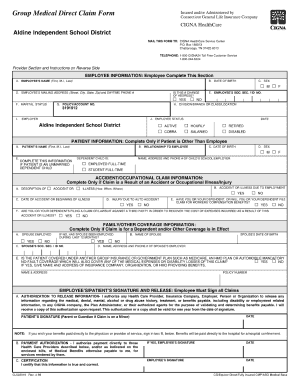
The Health Insurance Claim Form is essential in the healthcare process, specifically for submitting medical claims to insurance providers. It serves to communicate vital information regarding the patient and the services provided, ensuring timely payments for medical care. The CMS-1500 form is the standard version utilized in the U.S., making it an important document for healthcare professionals and patients alike.
This form is critical for both claim processing and treatment coverage, emphasizing the necessity of accurate completion and submission.
Purpose and Benefits of Using the Health Insurance Claim Form
The primary purpose of the Health Insurance Claim Form is to facilitate the claims submission process for medical services rendered. Understanding how to complete this form accurately can lead to several benefits:
-
Timely payments from insurance providers.
-
Reduced chances of claim denials.
-
Assured coverage for the medical services provided.
By utilizing the claim form correctly, users can significantly improve their healthcare reimbursement experience.
Who Needs to Complete the Health Insurance Claim Form?
Completion of the Health Insurance Claim Form is a collaborative effort involving several key roles:
-
Patient
-
Insured
-
Physician or Supplier
All parties listed must provide signatures to ensure payment authorization and the release of necessary medical information, highlighting the importance of teamwork in the claims process.
How to Fill Out the Health Insurance Claim Form: Step-by-Step Guide
Completing the Health Insurance Claim Form accurately can be straightforward if you follow these essential steps:
-
Begin with the Patient’s Name and the Insured’s Name.
-
Detail the relevant diagnoses and treatment dates.
-
List associated charges for each service rendered.
-
Ensure all required fields are filled out completely.
-
Review your entries for correctness and completeness.
This fillable form comes with fields and instructions to aid in filling it out correctly, helping avoid common errors and misunderstandings.
Common Errors in the Health Insurance Claim Form and How to Avoid Them
When filling out the Health Insurance Claim Form, users should be aware of frequent mistakes that can hinder claim processing. Commonly filled fields that may cause issues include:
-
Inaccurate Patient or Insured Names
-
Missing diagnosis codes
-
Incorrect dates of service
To minimize errors, it's recommended to use a validation checklist to review the form before submission, ensuring that all fields are accurately completed.
Submission Methods for the Health Insurance Claim Form
Once the Health Insurance Claim Form is completed, it can be submitted through various methods:
-
Online submission through an electronic claims processor.
-
Mailing it directly to the insurance provider's claims department.
After submission, confirming that the claim was received and tracking its status are essential steps to ensure successful processing.
What Happens After You Submit the Health Insurance Claim Form?
Submitting the Health Insurance Claim Form initiates a series of steps in the claims process:
-
The insurance provider reviews the submitted claim.
-
A decision is made regarding the claim's approval or denial.
-
Payments are issued based on the determination of coverage.
It's essential to be aware of typical processing times and wait for confirmation of receipt from the insurance provider to stay informed about the status of your claim.
Ensuring Security and Compliance While Submitting the Health Insurance Claim Form
When submitting the Health Insurance Claim Form, maintaining security and complying with regulations is crucial. Organizations implement various security measures, including:
-
256-bit encryption to protect sensitive information.
-
Compliance with HIPAA to safeguard patient privacy.
-
Adherence to GDPR standards when handling personal data.
Understanding these measures helps ensure that claims are handled discreetly and securely.
Use pdfFiller for Effortless Completion of the Health Insurance Claim Form
Utilizing pdfFiller can greatly simplify the process of filling out the Health Insurance Claim Form. Key features include:
-
Edit and complete form fields easily.
-
eSigning capabilities for quick authorization.
-
Document management tools to keep everything organized.
These capabilities make pdfFiller an invaluable resource for managing health insurance claims efficiently.
Sample Completed Health Insurance Claim Form
A sample completed Health Insurance Claim Form can serve as an excellent reference. This example provides:
-
A visual representation of a filled form.
-
Annotations explaining each field and its significance.
By reviewing a correctly completed claim, users can gain insights into the necessary information for successful claims submission.
How to fill out the CMS-1500 UB-04 CMS-1450 Package
-
1.Access the Health Insurance Claim Form on pdfFiller by searching for its name in the platform's template library or uploading it from your device.
-
2.Once the form is open, familiarize yourself with the layout and available fillable fields, such as 'Patient’s Name' and 'Insured’s Name.'
-
3.Before filling out the form, gather all necessary information, including patient details, dates of service, diagnoses, and charge amounts.
-
4.Use pdfFiller’s tools to click into each field and type or select the appropriate information. Ensure that you fill in all required fields marked clearly.
-
5.Double-check that each entry is accurate and matches the supporting documentation, such as invoices and medical records, to avoid common mistakes.
-
6.Once you've completed the form, carefully review it for any errors or missing information. Make any necessary corrections.
-
7.To finalize your submission, explore the options on the right-hand side of the pdfFiller interface. Here, you can save a copy of the completed form, download it in various formats, or submit it directly through email or a web portal.
Who is eligible to use the Health Insurance Claim Form?
Anyone who has received medical services and is looking to claim reimbursement from their health insurance provider can use this form. It includes patients, insured individuals, and healthcare providers.
What information is required to complete the claim form?
You will need the patient's personal information, insured party details, dates of service, medical codes, diagnoses, and the charges for services rendered to fill out the claim form properly.
How can I submit the Health Insurance Claim Form?
You can submit the form electronically via the insurance company’s online portal, or you may print it and mail it in. Be sure to check with your insurer for their specific submission requirements.
What are common mistakes to avoid when filling out the form?
Ensure all required fields are completed, and double-check that names, dates, and charges are accurate. Missing information or inaccuracies can delay processing and reimbursement.
How long does the processing of claims take?
Processing times may vary depending on the insurance provider. However, claims are typically processed within 30 days but can take longer if additional information is required.
Are there fees associated with submitting this form?
Generally, filling out and submitting the Health Insurance Claim Form does not incur a fee. However, you may want to verify with your insurance company for any specific processing fees that may apply.
Can the form be filled out online?
Yes, the Health Insurance Claim Form can be filled out online using platforms like pdfFiller, which provide fillable PDF features for ease of use.
Related Content
Related Forms

Related Catalogs

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.